Is the CXR technically good?
- Penetration - should be able to see spine through heart
- Underpenetrated - can't see spine; lung markings appear more prominent; L hemidiaphragm may not be distinguishable from lung base
- Overpenetrated - lung fields appear very dark, may look like pneumothorax (look for white pleural line) or emphysema (look for hyperinflation/flattened diaphragm)
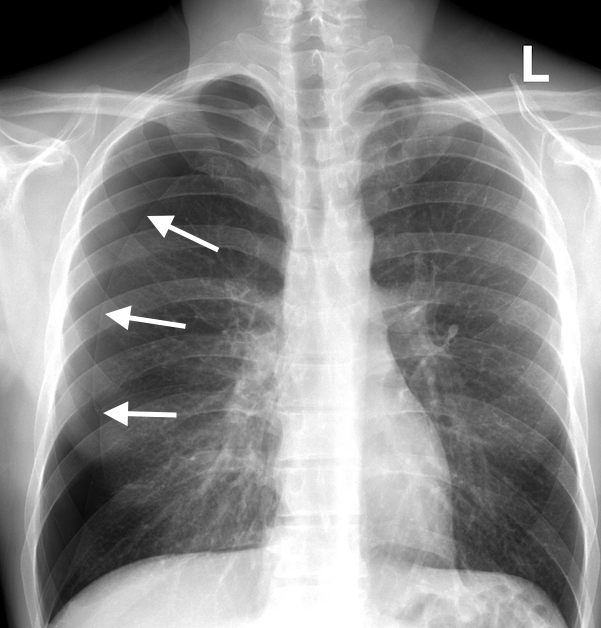
- Inspiration - should be able to see 8-9 posterior ribs (10 is excellent)
- Poor inspiration can compress lung bases and look like pneumonia; double check on the lateral view
- Rotation - spine should be centered between clavicles
- Spine closer to L medial clavicle - patient rotated towards right
- Spine closer to R medial clavicle - patient rotated towards left
- Rotation may distort hilar anatomy
- Magnification - heart appears slightly magnified on AP (portable) films
- Angulation - clavicle has S shape, and medial end superimposed on 3rd-4th ribs
- Clavicles closer to 1st rib - excessive angulation; may distort cardiac borders/obscure L hemidiaphragm
Endotracheal tube placement
- Tip of ETT should be 3-5 cm from the carina
- To estimate measurement, tube is typically 1 cm in diameter, and 3 cm is about 2 vertebral bodies
- Neck flexion can cause tube to descend 2 cm; extension can cause it to rise 2 cm
- Malpositioned tubes - most commonly in R mainstem bronchus (wider and straighter angle than L bronchus), which leads to atelectasis of the L lung and of non-aerated RUL
Pneumonia
- Usually homogenous density; air bronchograms may be present
- May see silhouette sign with lobar pneumonia
-
Obscured border Lobe Ascending aorta RUL R heart border RML R hemidiaphragm RLL Descending aorta LUL or LLL L heart border L lingula L hemidiaphragm LLL - Other hints for localization
- Spine sign on lateral view - normally thoracic spine appears whiter at top and blacker at bottom (x-ray traverses more bone tissue at the shoulders)
- More radioopaque/white spine indicates consolidated lung at that location
- CXR appearance will lag behind clinical improvement - takes days-weeks to resolve on imaging
| Appearance | Classic pathogen | |
| Lobar |
Homogeneous consolidation of lobe; air bronchograms may be present; silhouette signs or demarcation at fissures |
S. pneumo |
| Segmental |
Patchy, multifocal airspace disease with fluffy margins; no air bronchogram (bronchi filled w exudate); atelectasis |
S. aureus |
| Interstitial |
Fine reticular pattern, eventually becoming patchy/confluent |
Mycoplasma pneumonia; Pneumocystis pneumonia |
| Round | Round consolidation; typically in children; usually in posterior lower lobes | H. flu, strep, pneumococcus |
| Cavitary | Thin-walled with smooth margin, no air-fluid level | M. tuberculosis, staph |
| Aspiration | Dependent portion of lungs, R > L (due to straighter and wider R bronchus) | Not technically pneumonia since it is not infectious but more like pulmonary edema; gastric acid may cause chemical pneumonitis |



Pneumothorax
- Air in the pleural spaces causes visceral pleura to retract
- Diagnosis requires identification of visceral pleural white line
- Line will typically parallel the curve of the chest wall
- Absence of lung markings distal to line is frequent, but not sufficient to diagnose - may be due to bullae/cysts
- Presence of lung markings not sufficient to rule out
- Look-a-likes
- Skin fold - typically thicker than a pleural line
- Medial scapula border - trace the scapula and see if the 'pleural line' is separate from it
- Does it need a chest tube?
- Clinical status most important factor
- Note: size on CXR correlates poorly with actual size on CT and with degree of clinical impairment
- If distance between chest wall and the lung margin at the apex > 2 cm, usually requires chest tube drainage