Indications
- Prostate cancer screening
- Abnormal DRE - nodule or indurated area
- Abnormal total PSA (threshold generally > 4.0 ng/mL) (PSA increases with age, prostate trauma, GU infxn, ejaculation)
- Abnormal total PSA change:
- ≥ 0.35 ng/mL/yr [tPSA < 4]
- ≥ 0.75 ng/mL/yr [tPSA 4-10]
- Taking 5-ARI and PSA consistently rises by any amount, or does not decline ≥ 50% by 12 mo after starting 5-ARI
- Other screening tests to help decide if biopsy is warranted:
- % free PSA (see table below)
-
% free PSA Probability of cancer 0-10% 56% 10-15% 28% 15-20% 20% 20-25% 16% > 25% 8% - PCA3/MiPS(urine test after prostate massage)
- RNA-based test; used in men with elevated PSA + negative biopsy - if low, likely don't need repeat biopsy
- PHI (PSA-based score)
- 4K score (combines total/free PSA with kallikrein protein)
- Calculates % risk of any Gleason 7+ cancer. If ≥ 7.5%, consider biopsy
- Not valid if have taken 5-ARI in past 6 mo (lowers PSA).
- mpMRI
- PSA density > 0.10 ng/ml
Technique
- In-office procedure
- Use antibiotic prophylaxis (<24 hrs): oral FQ or IM/IV cephalosporin.
- Enema improves visibility but doesn't affect infection rate
- Prostate block with local anesthesia
- Target inferior hypogastric plexus along posterolateral prostate/near seminal vesicles - does not get below dentate line
- Transrectal ultrasound guidance (TRUS) for biopsy of 12 systematic cores
- 12 cores = (R and L) x (lateral and para-sagittal) x (apex, mid and base) of peripheral zone
- Additional lesion-directed cores (lesions appear hypoechoic; usually not seen)
- If previous negative biopsy, may also target transitional zone and anterior apical zone
- MRI fusion biopsy - combines prostate multi-parametric MRI (MP-MRI) with real-time ultrasound to target concerning lesions
- Indicated if had a previous negative biopsy - will detect PI-RADS 4-5 in 15-20% of these patients
- PPV 52%, NPV 92%
- MRI-guided biopsy + ipsilateral systematic biopsy catches 96% of cancers
- Can be done with 'cognitive' fusion or machine fusion
Transperineal biopsy
- Tape scrotum up with gown
- Chloraprep perineum
- Insert probe and mark injection points (line probe attachment up with perineal midline, and mark on either side)
- Anesthetize injection points (create small skin wheal then hub needle and inject deep), 10 cc on each side
- Put in trocar, tent skin to maintain the position but don't puncture skin, and inject local (20cc on each side. Anesthetize soft tissue and then the muscle (dump most of it in the muscle))
- After local injected, puncture skin with trocar and start taking biopsies
- Posterior right, anterior right, anterior left, posterior left
- Adjust trocar position for anterior vs posterior
Risks
- Minor hematuria/rectal bleeding/hematospermia.
- Major bleeding/infection are rare (1-2%).
Multiparametric MRI (mpMRI)
- High interobserver variability
- Should augment but not replace systematic biopsy
- Pre-biopsy screening: higher sensitivity, more effective in detecting clinically significant disease (compared to systematic biopsy); mpMRI could allow 25% to avoid a primary biopsy
- Consider for men with prior negative biopsy but continued PSA rise
- Positive mpMRI a/w 34-68% prostate cancer risk
PI-RADS
- Prostate lesion characterization on MRI
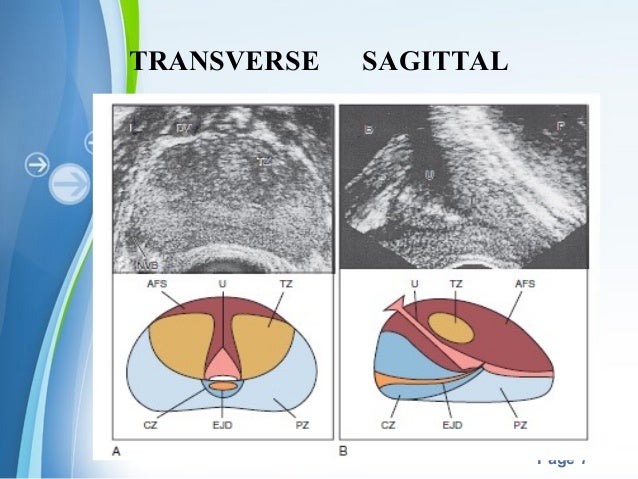
- MR pelvis anatomy
- Normal prostate on T2WI
- Peripheral zone (PZ) bright
- Transitional zone (TZ) heterogeneous ("organized chaos"), likely to see BPH nodules here
- Suspicious lesions are
- hypointense on T2
- bright on DWI (hypercellular/crowded, less diffusion), dark on ADC (apparent diffusion coefficient). Bright/bright might just be cyst.
- positive dynamic contrast enhancement (DCE) - early contrast enhancement compared to rest of prostate
- b value - factor that reflects the degree of diffusion weighting. Multiple b-values are acquired in sequence. Generally look at the higher b-value (1400-2000 s/mm2), it will have lower resolution but higher contrast
| PIRADS | T2WI (use for TZ) | DWI/ADC (use for PZ) | |
| 1 - very low | Uniform, hyperintense | Normal on DWI/ADC | |
| 2 - low | Linear, wedge-shaped, or diffuse mild hypointensity, usually indistinct margn | Indistinct hypointense on ADC | |
| 3 - intermediate | Heterogeneous intensity, or noncircumscribed, rounded, moderate hypointensity DWI = 5 makes this PI-RADS 4 |
Focal mild/moderate hypointense on ADC, isointense/mildly hyperintense on DWI + DCE makes this PI-RADS 4 |
|
| 4 - high | Circumscribed, homogeneous, moderate hypointense focus. Confined to prostate and < 1.5 cm in greatest dimension | Focal marked hypointense on ADC, marked hyperintense on DWI, < 1.5 cm on axial | |
| 5 - very high | 4 but ≥ 1.5 cm in greatest dimension, or definite extraprostatic extension/invasive behavior | 4 but ≥ 1.5 cm in greatest dimension, or definite extraprostatic extension/invasive behavior |